 | New Jersey Medical Power of Attorney Form |
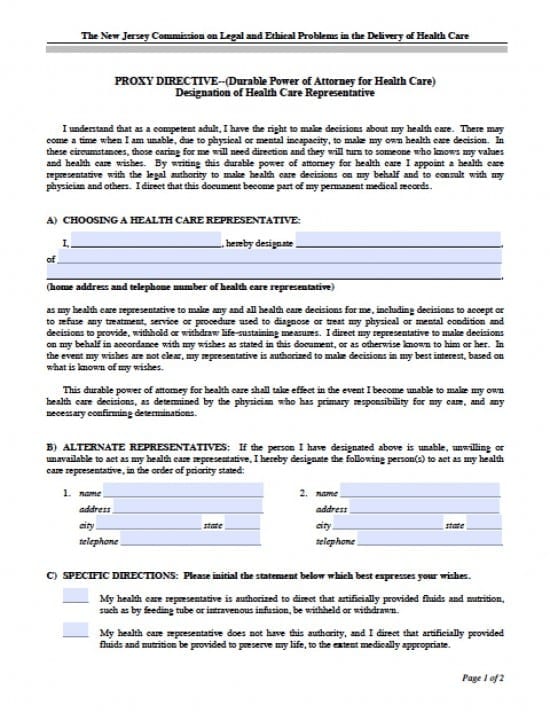
The New Jersey medical power of attorney form is a document that will a Principal shall use to provide powers and directives with regard to how they wish to have their health care handled if, in fact, they become unable to make their own decisions and/or communicate their own decisions to health care providers. The Principal should read through the document so that they are aware of what they will be signing. There is room for the Principal to be very direct in their decisions while they are of sound mind and they should be very clear in their direction to the Agent also making copies available to health care providers for their review to be certain the decisions made by an Agent are parallel if not exactly what the Principal’s expectations.
If the Principal is not clear of the statements contained within the document, they may wish to consider consulting with a knowledgeable attorney so that they may be more well educated about the inner workings of the document and any potential effects upon the Principal to be expected.
The Directive may be revoked at any time the Principal feels necessary. The notice must be in writing and delivered to the Agent or by assigning a new document to a new Agent in which case the current document will be immediately (according to the date entered in the revocation) be revoked.
How to Write
Step 1 – Designation of Agent by Principal –
The Principal must download the document and begin by reading the introduction prior to proceeding with completion and signature of the document:
- Submit the Principal’s full name
- Designate the Agent by entering their full name
- Enter the Agent’s address
- Telephone number of the health care provider
- Principal must review the remainder of this section
Step 2 – Alternate Representatives (Agent’s) –
In the event the initial designee is no longer available to serve, the Principal may provide the names of alternate Agent(s) – Submit the following information:
- Alternate(s) Name(s)
- Addresses
- City
- State
- Telephone Number(s)
Step 3 – Specific Instructions –
The Principal must review both statements as follows, on the form, and initial the statement that best indicates their wishes:
- My health care representative is authorized to direct that artificially provided fluids and nutrition, such as by feeding tube or intravenous infusion, be withheld or withdrawn.
- OR
- My health care representative does not have this authority, and I direct that artificially provided fluids and nutrition be provided to preserve my life, to the extent medically appropriate.
Specific Instruction –
- Should the Principal choose to add other specific instructions, they may do so in the lines provided on the form
Step 4 – Copies –
The Principal shall provide the original copy of the document to the initial Agent:
- Copies must be provided to any Alternates
- The Principal must also retain a copy for their own records
- To ensure that their health care providers are aware of their wishes, provide copies to primary care physicians, hospice staff and hospital records
Step 5 – Principal’s Signature –
The Principal must carefully read the paragraph at the beginning of this section. If in agreement, submit the following:
- Date this document in dd/mm/yyyy format
- The Principal’s signature
- Full address
- City, State
Step 6 – Witnesses Signatures and Information –
The Witnesses must review the paragraph prior to submitting the following:
- Witnesses Signatures
- Witnesses Addresses
- City, State
- Witnesses Signatures
- Date of signatures in mm/dd/yyyy format